Adoption should be the ONLY OPTION:
PLEASE, CONSIDER ADOPTION. Not only for the sake of the
life growing inside you, but for your OWN WELL-BEING.
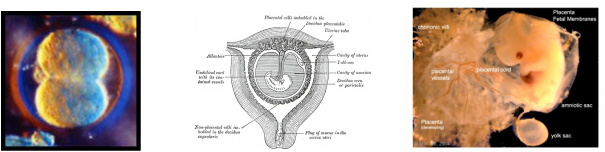
First Picture: 30 hours after conception.
Second Picture: Week 2.
Third Picture: Week 3.
When does life begin?
Fertilization: LIFE BEGINS!
Life begins at fertilization, when the sperm and the female egg cell or ovum, meet to form a single cell. A new human life is created, different from his/her mother or father, different from any human being that has ever lived or ever will live. This new human life is totally unique, pre-destined by God Himself, and has his/her own genetic code that will determine the characteristics he/she will have for the rest of his/her life.
Within one week of fertilization, the new human implants in the mother's uterus and is nourished there for the next nine months.
At three weeks, the baby's heart begins to beat. A microscope would reveal that this little baby has the characteristic 46 human chromosomes in every cell, demonstrating clearly that this is a human being.
At 6 weeks, the baby has brain waves that can be measured with an electroencephalogram.
This 8 week old unborn baby swims freely in the amniotic sac with a natural swimmer's stroke. The mother won't feel him yet though until about 4 1/2 months into the pregnancy.
At this age the baby is approximately the length of your thumb.
He/she responds to painful stimuli, such as a needle prick, will grasp an object and make a fist.
Each organ is present. The heart beats sturdily, the stomach provides digestive juices, the liver makes blood cells and the kidneys begin to function.
At 12 Weeks, the baby is very active! He/she can kick his legs, curl his toes, squint, turn his head, open his mouth and swallow.
By 16 weeks, the baby is 13.97cm (5 1/2 inches) long and weighs nearly a pound. Fine details of development are present such as fingernails and eyelashes.
Throughout his time in-utero, the unborn child is nourished with food, water and oxygen by his mother through the placenta.
At 18 weeks, the baby’s nostrils and toenails become visible. The baby may suck his/her thumb, turn somersaults, and has a firm grip. The ovaries of girls contain the beginnings of eggs. She begins to develop her own sleeping habits.
By 20 weeks, unborn children are capable of feeling pain and likely feel pain much earlier. Dr. Maureen Condic, an expert on human embryonic development and Associate Professor of Neurobiology and Anatomy at the University of Utah, has testified that the neural circuitry responsible for the most primitive response to pain, the spinal reflex, is in place by 8 weeks of development.
By 22 weeks, the baby is kicking, turning, and hiccuping. Mom may be able to identify a bulge as an elbow or the baby’s head. The testes descend in boys. At this point in the pregnancy, each side of the brain has a billion nerve cells.
At 26 weeks, the child sleeps in her favourite positions, and stretches upon waking up.
By weeks 27, the baby will be able to hear.
At 30 weeks, the baby weighs about 1.58kg (3 lbs, 5 oz). Her eyelids begin to open and close, preparing her to see outside the womb. Even her eyelashes are developed.
At 34 weeks, the child’s skin becomes pink and smooth.
The pupils of her eyes respond to light, and her fingernails reach right to the tip of her fingers. Measuring about 30.48cm (12 inches) and weighing about 2.26kg (5 lbs), the baby is really getting cramped now.
At 38-40 weeks, the baby triggers labour and is born, usually from 264-270 days after conception.
http://www.abortionclinics.ca/is-it-really-a-baby.shtml
Fertilization: LIFE BEGINS!
Life begins at fertilization, when the sperm and the female egg cell or ovum, meet to form a single cell. A new human life is created, different from his/her mother or father, different from any human being that has ever lived or ever will live. This new human life is totally unique, pre-destined by God Himself, and has his/her own genetic code that will determine the characteristics he/she will have for the rest of his/her life.
Within one week of fertilization, the new human implants in the mother's uterus and is nourished there for the next nine months.
At three weeks, the baby's heart begins to beat. A microscope would reveal that this little baby has the characteristic 46 human chromosomes in every cell, demonstrating clearly that this is a human being.
At 6 weeks, the baby has brain waves that can be measured with an electroencephalogram.
This 8 week old unborn baby swims freely in the amniotic sac with a natural swimmer's stroke. The mother won't feel him yet though until about 4 1/2 months into the pregnancy.
At this age the baby is approximately the length of your thumb.
He/she responds to painful stimuli, such as a needle prick, will grasp an object and make a fist.
Each organ is present. The heart beats sturdily, the stomach provides digestive juices, the liver makes blood cells and the kidneys begin to function.
At 12 Weeks, the baby is very active! He/she can kick his legs, curl his toes, squint, turn his head, open his mouth and swallow.
By 16 weeks, the baby is 13.97cm (5 1/2 inches) long and weighs nearly a pound. Fine details of development are present such as fingernails and eyelashes.
Throughout his time in-utero, the unborn child is nourished with food, water and oxygen by his mother through the placenta.
At 18 weeks, the baby’s nostrils and toenails become visible. The baby may suck his/her thumb, turn somersaults, and has a firm grip. The ovaries of girls contain the beginnings of eggs. She begins to develop her own sleeping habits.
By 20 weeks, unborn children are capable of feeling pain and likely feel pain much earlier. Dr. Maureen Condic, an expert on human embryonic development and Associate Professor of Neurobiology and Anatomy at the University of Utah, has testified that the neural circuitry responsible for the most primitive response to pain, the spinal reflex, is in place by 8 weeks of development.
By 22 weeks, the baby is kicking, turning, and hiccuping. Mom may be able to identify a bulge as an elbow or the baby’s head. The testes descend in boys. At this point in the pregnancy, each side of the brain has a billion nerve cells.
At 26 weeks, the child sleeps in her favourite positions, and stretches upon waking up.
By weeks 27, the baby will be able to hear.
At 30 weeks, the baby weighs about 1.58kg (3 lbs, 5 oz). Her eyelids begin to open and close, preparing her to see outside the womb. Even her eyelashes are developed.
At 34 weeks, the child’s skin becomes pink and smooth.
The pupils of her eyes respond to light, and her fingernails reach right to the tip of her fingers. Measuring about 30.48cm (12 inches) and weighing about 2.26kg (5 lbs), the baby is really getting cramped now.
At 38-40 weeks, the baby triggers labour and is born, usually from 264-270 days after conception.
http://www.abortionclinics.ca/is-it-really-a-baby.shtml
What is the duration of a pregnancy?
A normal pregnancy can last from 245 to 270 days from conception to delivery, the average being 266 days. If you are counting from the last period add 14 days to these numbers.
When are you most likely to fall pregnant?
Ovulation occurs around 12-14 days after period and for 2 days a woman is open to fertilization. Period is a consequence of ovulation during which a uterine lining is created for the possible pregnancy. When pregnancy doesn’t occur, we shed this lining and this is what we call periods. Ovulation occurs variably in different women.
Jargon explained:
Preterm, term and post term:
Pregnancy is considered "at term" when gestation has lasted 37 complete weeks (occurring at the transition from the 37th to the 38th week of gestation), but is less than 42 weeks of gestational age (occurring at the transition from the 42nd week to the 43rd week of gestation, or between 259 and 294 days since LMP). "Full term" refers to the gestation having lasted 40 weeks from the first day of the mother's last menstrual period. This is the end of gestation on average. Alternatively expressed, this corresponds to a gestational age of 40 weeks and 0 days, or 280 days, or approximately 9 months, and occurs at the transition from the 40th to the 41st week of gestation. On average, it corresponds to an embryonic age of 38 weeks or 266 days.
Events before completion of 37 weeks (259 days) are considered preterm; from week 42 (294 days) events are considered post term. When a pregnancy exceeds 42 weeks (294 days), the risk of complications for both the woman and the fetus increases significantly. Therefore, in an otherwise uncomplicated pregnancy, obstetricians usually prefer to induce labour at some stage between 41 and 42 weeks.
Birth before 39 weeks by C section, even if considered "at term", results in an increases risk of complications and premature death, when not medically needed. This is from factors including underdeveloped lungs, infection due to underdeveloped immune system, problems feeding due to underdeveloped brain, and jaundice from underdeveloped liver. Some hospitals in the United States have noted a significant increase in neonatal intensive care unit patients when women schedule deliveries for convenience and are taking steps to reduce induction for non-medical reasons. Complications from Caesarean section are more common than for live births.
Recent medical literature prefers the terminology preterm and post term to premature and post mature. Preterm and post term are unambiguously defined as above, whereas premature and post mature have historical meaning and relate more to the infant's size and state of development rather than to the stage of pregnancy
Diagnosis
The beginning of pregnancy may be detected either based on symptoms by the pregnant woman herself, or by using medical tests with or without the assistance of a medical professional. Approximately 1 in 475 women at 20 weeks, and 1 in 2500 women at delivery, refuse to acknowledge that they are pregnant, which is called denial of pregnancy. Some non-pregnant women have a very strong belief that they are pregnant along with some of the physical changes. This condition is known as pseudocyesis or false pregnancy.
Physical signs
Most pregnant women experience a number of symptoms, which can signify pregnancy. The symptoms can include nausea and vomiting, excessive tiredness and fatigue, cravings for certain foods that are not normally sought out, and frequent urination particularly during the night.
A number of early medical signs are associated with pregnancy These signs typically appear, if at all, within the first few weeks after conception. Although not all of these signs are universally present, nor are all of them diagnostic by themselves, taken together they make a presumptive diagnosis of pregnancy. These signs include the presence of human chorionic gonadotropin (hCG) in the blood and urine, missed menstrual period, implantation bleeding that occurs at implantation of the embryo in the uterus during the third or fourth week after last menstrual period, increased basal body temperature sustained for over 2 weeks after ovulation, Chadwick's sign (darkening of the cervix, vagina, and vulva), Goodell's sign (softening of the vaginal portion of the cervix), Hegar's sign (softening of the uterus isthmus), and pigmentation of linea alba – Linea nigra, (darkening of the skin in a mid-line of the abdomen, caused by hyper-pigmentation resulting from hormonal changes, usually appearing around the middle of pregnancy) Breast tenderness is common during the first trimester, and is more common in women who are pregnant at a young age.
Despite all the signs, some women may not realize they are pregnant until they are far along in pregnancy. In some cases, a few have not been aware of their pregnancy until they begin labour. This can be caused by many factors, including irregular periods (quite common in teenagers), certain medications (not related to conceiving children), and obese women who disregard their weight gain. Others may be in denial of their situation.
Tests Pregnancy detection can be accomplished using one or more various pregnancy tests, which detect hormones generated by the newly formed placenta. Blood and urine tests can detect pregnancy 12 days after implantation. Blood pregnancy tests are more sensitive than urine tests (giving fewer false negatives). Home pregnancy tests are urine tests, and normally detect a pregnancy 12 to 15 days after fertilization. A quantitative blood test can determine approximately the date the embryo was conceived. Testing 48 hours apart can provide useful information regarding how the pregnancy is doing. A single test of progesterone levels can also help determine how likely a fetus will survive in those with a threatened miscarriage (bleeding in early pregnancy).
An early obstetric ultrasonography can determine the age of the pregnancy fairly accurately. In practice, medical professionals typically express the age of a pregnancy (i.e., an "age" for an embryo) in terms of "menstrual date" based on the first day of a woman's last menstrual period, as the woman reports it. Unless a woman's recent sexual activity has been limited, she has been charting her cycles, or the conception is the result of some types of fertility treatment (such as IUI or IVF), the exact date of fertilization is unknown. Without symptoms such as morning sickness, often the only visible sign of a pregnancy is an interruption of the woman's normal monthly menstruation cycle, (i.e., a "late period"). Hence, the "menstrual date" is simply a common educated estimate for the age of a fetus, which is an average of 2 weeks later than the first day of the woman's last menstrual period. The term "conception date" may sometimes be used when that date is more certain, though even medical professionals can be imprecise with their use of the two distinct terms. The due date can be calculated by using Naegele's rule. The expected date of delivery may also be calculated from sonogram measurement of the fetus. This method is slightly more accurate than methods based on LMP. Additional obstetric diagnostic techniques can estimate the health and presence or absence of congenital diseases at an early stage.
Ultrasound See also: Obstetric ultrasonography
One way to observe prenatal development is via ultrasound images. Ultrasound imaging before 24 weeks can help determine the due date and detect multiple pregnancies however in those who are at low risk it is unclear if this makes a significant difference in outcomes. Routine ultrasound imaging after 24 weeks gestation does not improve outcomes in either the mother or the baby and might increase the risk of a cesarean section. It is thus is not recommended. Modern 3D ultrasound images provide greater detail for prenatal diagnosis than the older 2D ultrasound technology. While 3D is popular with parents desiring a prenatal photograph as a keepsake, both 2D and 3D are discouraged by the FDA for non-medical use, but there are no definitive studies linking ultrasound to any adverse medical effects
A normal pregnancy can last from 245 to 270 days from conception to delivery, the average being 266 days. If you are counting from the last period add 14 days to these numbers.
When are you most likely to fall pregnant?
Ovulation occurs around 12-14 days after period and for 2 days a woman is open to fertilization. Period is a consequence of ovulation during which a uterine lining is created for the possible pregnancy. When pregnancy doesn’t occur, we shed this lining and this is what we call periods. Ovulation occurs variably in different women.
Jargon explained:
Preterm, term and post term:
Pregnancy is considered "at term" when gestation has lasted 37 complete weeks (occurring at the transition from the 37th to the 38th week of gestation), but is less than 42 weeks of gestational age (occurring at the transition from the 42nd week to the 43rd week of gestation, or between 259 and 294 days since LMP). "Full term" refers to the gestation having lasted 40 weeks from the first day of the mother's last menstrual period. This is the end of gestation on average. Alternatively expressed, this corresponds to a gestational age of 40 weeks and 0 days, or 280 days, or approximately 9 months, and occurs at the transition from the 40th to the 41st week of gestation. On average, it corresponds to an embryonic age of 38 weeks or 266 days.
Events before completion of 37 weeks (259 days) are considered preterm; from week 42 (294 days) events are considered post term. When a pregnancy exceeds 42 weeks (294 days), the risk of complications for both the woman and the fetus increases significantly. Therefore, in an otherwise uncomplicated pregnancy, obstetricians usually prefer to induce labour at some stage between 41 and 42 weeks.
Birth before 39 weeks by C section, even if considered "at term", results in an increases risk of complications and premature death, when not medically needed. This is from factors including underdeveloped lungs, infection due to underdeveloped immune system, problems feeding due to underdeveloped brain, and jaundice from underdeveloped liver. Some hospitals in the United States have noted a significant increase in neonatal intensive care unit patients when women schedule deliveries for convenience and are taking steps to reduce induction for non-medical reasons. Complications from Caesarean section are more common than for live births.
Recent medical literature prefers the terminology preterm and post term to premature and post mature. Preterm and post term are unambiguously defined as above, whereas premature and post mature have historical meaning and relate more to the infant's size and state of development rather than to the stage of pregnancy
Diagnosis
The beginning of pregnancy may be detected either based on symptoms by the pregnant woman herself, or by using medical tests with or without the assistance of a medical professional. Approximately 1 in 475 women at 20 weeks, and 1 in 2500 women at delivery, refuse to acknowledge that they are pregnant, which is called denial of pregnancy. Some non-pregnant women have a very strong belief that they are pregnant along with some of the physical changes. This condition is known as pseudocyesis or false pregnancy.
Physical signs
Most pregnant women experience a number of symptoms, which can signify pregnancy. The symptoms can include nausea and vomiting, excessive tiredness and fatigue, cravings for certain foods that are not normally sought out, and frequent urination particularly during the night.
A number of early medical signs are associated with pregnancy These signs typically appear, if at all, within the first few weeks after conception. Although not all of these signs are universally present, nor are all of them diagnostic by themselves, taken together they make a presumptive diagnosis of pregnancy. These signs include the presence of human chorionic gonadotropin (hCG) in the blood and urine, missed menstrual period, implantation bleeding that occurs at implantation of the embryo in the uterus during the third or fourth week after last menstrual period, increased basal body temperature sustained for over 2 weeks after ovulation, Chadwick's sign (darkening of the cervix, vagina, and vulva), Goodell's sign (softening of the vaginal portion of the cervix), Hegar's sign (softening of the uterus isthmus), and pigmentation of linea alba – Linea nigra, (darkening of the skin in a mid-line of the abdomen, caused by hyper-pigmentation resulting from hormonal changes, usually appearing around the middle of pregnancy) Breast tenderness is common during the first trimester, and is more common in women who are pregnant at a young age.
Despite all the signs, some women may not realize they are pregnant until they are far along in pregnancy. In some cases, a few have not been aware of their pregnancy until they begin labour. This can be caused by many factors, including irregular periods (quite common in teenagers), certain medications (not related to conceiving children), and obese women who disregard their weight gain. Others may be in denial of their situation.
Tests Pregnancy detection can be accomplished using one or more various pregnancy tests, which detect hormones generated by the newly formed placenta. Blood and urine tests can detect pregnancy 12 days after implantation. Blood pregnancy tests are more sensitive than urine tests (giving fewer false negatives). Home pregnancy tests are urine tests, and normally detect a pregnancy 12 to 15 days after fertilization. A quantitative blood test can determine approximately the date the embryo was conceived. Testing 48 hours apart can provide useful information regarding how the pregnancy is doing. A single test of progesterone levels can also help determine how likely a fetus will survive in those with a threatened miscarriage (bleeding in early pregnancy).
An early obstetric ultrasonography can determine the age of the pregnancy fairly accurately. In practice, medical professionals typically express the age of a pregnancy (i.e., an "age" for an embryo) in terms of "menstrual date" based on the first day of a woman's last menstrual period, as the woman reports it. Unless a woman's recent sexual activity has been limited, she has been charting her cycles, or the conception is the result of some types of fertility treatment (such as IUI or IVF), the exact date of fertilization is unknown. Without symptoms such as morning sickness, often the only visible sign of a pregnancy is an interruption of the woman's normal monthly menstruation cycle, (i.e., a "late period"). Hence, the "menstrual date" is simply a common educated estimate for the age of a fetus, which is an average of 2 weeks later than the first day of the woman's last menstrual period. The term "conception date" may sometimes be used when that date is more certain, though even medical professionals can be imprecise with their use of the two distinct terms. The due date can be calculated by using Naegele's rule. The expected date of delivery may also be calculated from sonogram measurement of the fetus. This method is slightly more accurate than methods based on LMP. Additional obstetric diagnostic techniques can estimate the health and presence or absence of congenital diseases at an early stage.
Ultrasound See also: Obstetric ultrasonography
One way to observe prenatal development is via ultrasound images. Ultrasound imaging before 24 weeks can help determine the due date and detect multiple pregnancies however in those who are at low risk it is unclear if this makes a significant difference in outcomes. Routine ultrasound imaging after 24 weeks gestation does not improve outcomes in either the mother or the baby and might increase the risk of a cesarean section. It is thus is not recommended. Modern 3D ultrasound images provide greater detail for prenatal diagnosis than the older 2D ultrasound technology. While 3D is popular with parents desiring a prenatal photograph as a keepsake, both 2D and 3D are discouraged by the FDA for non-medical use, but there are no definitive studies linking ultrasound to any adverse medical effects
Amniocentesis:
Everything You Need to Know About Amniocentesis
By Bette Van Metter, CNM, MSN - January 1, 1999
What is amniocentesis?
Amniocentesis provides genetic information about the fetus -- as well as information about its health and maturity -- through the removal of a small sample of amniotic fluid. A needle is inserted through the pregnant woman’s abdominal wall, uterine wall and amniotic sac to withdraw fluid which contains cells that have been shed by the fetus. Those cells are then cultured and analyzed. Amniocentesis can be performed during either the second or third trimester, depending on the reason it is being done. Amniocentesis for genetic diagnosis is most commonly performed between 15 and 18 weeks’ gestation.
What does this procedure entail?
For several hours prior to the amniocentesis, the woman should drink plenty of fluids to ensure an adequate volume of amniotic fluid during the procedure. The test does not require a full bladder. An ultrasound prior to the procedure determines the fetal age, position of the fetus, location of the placenta, fetal heartbeat and the number of fetuses. An ultrasound transducer (a device which delivers the ultrasound scan) remains in place to guide the needle and prevent puncturing of the placenta, fetus and umbilical cord.
The woman's abdomen is washed with a sterile solution and sterile drapes are placed over the area. A local anesthetic is not commonly used since this requires an additional needle insertion. Approximately 15 to 30 ml (1 1/2 to 3 tablespoons) of amniotic fluid is withdrawn. Withdrawal of the fluid takes about two minutes, and the body replaces it within about 12 hours of the procedure. Care is taken when extracting this fluid to avoid contamination of the sample with maternal blood, which would invalidate the results.
Everything You Need to Know About Amniocentesis
By Bette Van Metter, CNM, MSN - January 1, 1999
What is amniocentesis?
Amniocentesis provides genetic information about the fetus -- as well as information about its health and maturity -- through the removal of a small sample of amniotic fluid. A needle is inserted through the pregnant woman’s abdominal wall, uterine wall and amniotic sac to withdraw fluid which contains cells that have been shed by the fetus. Those cells are then cultured and analyzed. Amniocentesis can be performed during either the second or third trimester, depending on the reason it is being done. Amniocentesis for genetic diagnosis is most commonly performed between 15 and 18 weeks’ gestation.
What does this procedure entail?
For several hours prior to the amniocentesis, the woman should drink plenty of fluids to ensure an adequate volume of amniotic fluid during the procedure. The test does not require a full bladder. An ultrasound prior to the procedure determines the fetal age, position of the fetus, location of the placenta, fetal heartbeat and the number of fetuses. An ultrasound transducer (a device which delivers the ultrasound scan) remains in place to guide the needle and prevent puncturing of the placenta, fetus and umbilical cord.
The woman's abdomen is washed with a sterile solution and sterile drapes are placed over the area. A local anesthetic is not commonly used since this requires an additional needle insertion. Approximately 15 to 30 ml (1 1/2 to 3 tablespoons) of amniotic fluid is withdrawn. Withdrawal of the fluid takes about two minutes, and the body replaces it within about 12 hours of the procedure. Care is taken when extracting this fluid to avoid contamination of the sample with maternal blood, which would invalidate the results.
Other forms of screening for abnormalities:
Screening with Maternal Blood
Blood being drawn from a pregnant woman for AFP and other fetal chemical screening
A much more routinely done diagnostic procedure for pregnant women is testing their blood for alpha-feto protein and several other chemicals originating from their fetus. This screening is significantly less expensive and has no risk of causing a miscarriage. However, the information gained is less reliable in predicting a chromosomal abnormality. Therefore, positive AFP results are usually followed up by amniocentesis for verification.
Alpha-feto protein is a substance normally produced by the liver of fetuses and is carried in their blood. Some of the fetal blood leaks into the placenta and then into the mother's blood during pregnancy. The AFP, and other diagnostic fetal and maternal chemicals, can be separated from a blood sample taken from the mother's arm. Unusually high or low amounts of AFP relative to the stage of pregnancy indicate that there may be particular kinds of genetic defects. Specifically, it may indicate the likelihood of Down syndrome, neural tube defects, abdominal wall defects, and trisomy 18 .
AFP testing is routinely done in the 14th to 20th week of a pregnancy. If the date of conception has been miscalculated, a false positive test result can occur. A similar error can happen if it is unknown that there are twins, because two fetuses produce more AFP than one.
Other substances of fetal origin found in a mother's blood that are commonly tested for in addition to AFP are the hormones HCG (human chorionic gonadotropin) and unconjugated estriol. The combined testing procedure is referred to as Alpha-fetoprotein Plus or triple screening. Recently, testing for inhibin has also been added to the combined screening. Subsequently, the test is referred to as quadruple or quad screening. The American College of Obstetricians and Gynecologists guidelines now recommend that all pregnant women have triple screening blood tests and ultrasound testing in the first trimester of their pregnancies.
NOTE: Human chorionic gonadotropin is produced by the embryo and later in a pregnancy by the placenta. Unconjugated estriol is a form of estrogen that is made by the liver of the fetus and by the placenta. Inhibin-A is a hormone that plays a part in regulating the menstrual cycle. It is produced normally by the ovaries but also by the placenta during a pregnancy. A newer diagnostic blood test used by some doctors looks for the presence of PAPPA (pregnancy-associated plasma protein A). Still another new test (MaterniT21 LTD) that also involves sampling maternal blood is likely to prove the most reliable for diagnosing Down syndrome. Unlike the other procedures, it does not look for fetal proteins but rather for fetal DNA. Early indications are that it may be 99.1% accurate and have a low false positive rate.
High-resolution Sonogram Screening
The near future of pregnancy screening for birth defects is likely to focus on the new generation of high-resolution ultrasound devices that are now becoming available. They are beginning to be used by doctors who have been specially trained to detect the early anatomical signs associated with some abnormalities. Using this procedure, Down syndrome can be reliably detected in the first trimester of a pregnancy. In addition, it is possible to detect structural defects such as brain cysts and cleft-palates. An advantage of high-resolution sonograms for screening is that they do not increase the risk of miscarriage and can be done early in a pregnancy. In addition, they are relatively inexpensive and quick since there are no samples to be processed in a laboratory. However, it is unlikely in the near future that amniocentesis will stop being considered the gold standard for detecting chromosomal abnormalities.
Screening for Abnormal DNA and RNA Sequences
Somewhat further in the future will be prenatal blood tests to find and analyze a wide range of abnormal fetal DNA and RNA sequences found in a pregnant woman's blood. Such tests would have the advantages of being relatively inexpensive and noninvasive while providing highly accurate results. One such diagnostic procedure to discover Down syndrome, called MaterniT21, has been developed and is being tested now. Early results indicate that it may be 99.1% accurate with no risk for the fetus. This and other tests may largely replace amniocentesis in the future.
Finding Disease Genes--from the PBS Nova series video Cracking the Code of Life
This link takes you to an external website. To return here, you must click the
"back" button on your browser program. (length = 9 mins, 27 secs)
NOTE: additional tests for 24-29 mostly rare genetic and metabolic diseases are now routinely done with a little blood taken from the heel of newborn babies. These tests are mandated by law in all 50 U.S. states. One such test is for detecting phenylketonuria (PKU), an inherited disorder that causes mental retardation and other neurological problems.
http://anthro.palomar.edu/abnormal/abnormal_2.htm
Screening with Maternal Blood
Blood being drawn from a pregnant woman for AFP and other fetal chemical screening
A much more routinely done diagnostic procedure for pregnant women is testing their blood for alpha-feto protein and several other chemicals originating from their fetus. This screening is significantly less expensive and has no risk of causing a miscarriage. However, the information gained is less reliable in predicting a chromosomal abnormality. Therefore, positive AFP results are usually followed up by amniocentesis for verification.
Alpha-feto protein is a substance normally produced by the liver of fetuses and is carried in their blood. Some of the fetal blood leaks into the placenta and then into the mother's blood during pregnancy. The AFP, and other diagnostic fetal and maternal chemicals, can be separated from a blood sample taken from the mother's arm. Unusually high or low amounts of AFP relative to the stage of pregnancy indicate that there may be particular kinds of genetic defects. Specifically, it may indicate the likelihood of Down syndrome, neural tube defects, abdominal wall defects, and trisomy 18 .
AFP testing is routinely done in the 14th to 20th week of a pregnancy. If the date of conception has been miscalculated, a false positive test result can occur. A similar error can happen if it is unknown that there are twins, because two fetuses produce more AFP than one.
Other substances of fetal origin found in a mother's blood that are commonly tested for in addition to AFP are the hormones HCG (human chorionic gonadotropin) and unconjugated estriol. The combined testing procedure is referred to as Alpha-fetoprotein Plus or triple screening. Recently, testing for inhibin has also been added to the combined screening. Subsequently, the test is referred to as quadruple or quad screening. The American College of Obstetricians and Gynecologists guidelines now recommend that all pregnant women have triple screening blood tests and ultrasound testing in the first trimester of their pregnancies.
NOTE: Human chorionic gonadotropin is produced by the embryo and later in a pregnancy by the placenta. Unconjugated estriol is a form of estrogen that is made by the liver of the fetus and by the placenta. Inhibin-A is a hormone that plays a part in regulating the menstrual cycle. It is produced normally by the ovaries but also by the placenta during a pregnancy. A newer diagnostic blood test used by some doctors looks for the presence of PAPPA (pregnancy-associated plasma protein A). Still another new test (MaterniT21 LTD) that also involves sampling maternal blood is likely to prove the most reliable for diagnosing Down syndrome. Unlike the other procedures, it does not look for fetal proteins but rather for fetal DNA. Early indications are that it may be 99.1% accurate and have a low false positive rate.
High-resolution Sonogram Screening
The near future of pregnancy screening for birth defects is likely to focus on the new generation of high-resolution ultrasound devices that are now becoming available. They are beginning to be used by doctors who have been specially trained to detect the early anatomical signs associated with some abnormalities. Using this procedure, Down syndrome can be reliably detected in the first trimester of a pregnancy. In addition, it is possible to detect structural defects such as brain cysts and cleft-palates. An advantage of high-resolution sonograms for screening is that they do not increase the risk of miscarriage and can be done early in a pregnancy. In addition, they are relatively inexpensive and quick since there are no samples to be processed in a laboratory. However, it is unlikely in the near future that amniocentesis will stop being considered the gold standard for detecting chromosomal abnormalities.
Screening for Abnormal DNA and RNA Sequences
Somewhat further in the future will be prenatal blood tests to find and analyze a wide range of abnormal fetal DNA and RNA sequences found in a pregnant woman's blood. Such tests would have the advantages of being relatively inexpensive and noninvasive while providing highly accurate results. One such diagnostic procedure to discover Down syndrome, called MaterniT21, has been developed and is being tested now. Early results indicate that it may be 99.1% accurate with no risk for the fetus. This and other tests may largely replace amniocentesis in the future.
Finding Disease Genes--from the PBS Nova series video Cracking the Code of Life
This link takes you to an external website. To return here, you must click the
"back" button on your browser program. (length = 9 mins, 27 secs)
NOTE: additional tests for 24-29 mostly rare genetic and metabolic diseases are now routinely done with a little blood taken from the heel of newborn babies. These tests are mandated by law in all 50 U.S. states. One such test is for detecting phenylketonuria (PKU), an inherited disorder that causes mental retardation and other neurological problems.
http://anthro.palomar.edu/abnormal/abnormal_2.htm
